Top 3 Requirements for Payer-to-Payer Data Exchange
3.21.2024
On January 17, 2024, the Centers for Medicare & Medicaid Services (CMS) finalized the Interoperability and Prior Authorization Final Rule. One of the requirements under the Rule is Payer-to-Payer Data Exchange. This mandate requires select Medicare Advantage and Medicaid entities to exchange member data (at the request of a member) with other payers using a Payer-to-Payer application programing interface (API).
The Final Rule marks significant progress toward ensuring that health plans and providers have access to the member data necessary for treatment plans based on up-to-date and accurate information. With the looming January 1, 2027, mandatory enforcement date, some health plans are still in the process of uncovering the most effective way to comply with the requirements and position themselves for future success.
At Availity, we understand the complexity of trying to facilitate data exchange across multiple data standard types and systems. To assist your health plan in achieving compliance, we’ve highlighted the top three requirements for payer-to-payer data exchange and outlined an easy-to-follow guide.1
Affected health plans will need to establish and maintain Payer-to-Payer APIs. These APIs will facilitate the exchange of member data with other payers using a very similar interface to the Patient Access API that payers have already been working on. The Payer-to-Payer API has the distinction from Patient Access, which can exclude provider remittances and patient cost-sharing information. The exchanged data will encompass all data classes and elements specified in the U.S. Core Data for Interoperability (USCDI) version 1 content standard, along with specific details about the patient’s prior authorizations.
Payer-to-payer transactions starts with a member-initiated request to the former payer for releasing clinical healthcare data to the current payer. This request may be made through a member app, the former payer’s website, or a customer service call. The former payer, upon initiation, needs to identify and validate the former member. Some systems may require new web pages for inactive members to access information.
This process could lead to an increase in customer service calls. Initially, we identify the former member, complete HIPAA security validations, and confirm the destination of the current health plan. Then, we package and transmit the former member’s data to the current payer.
Figure one is a Venn diagram demonstrating that only two out of the six standards overlap across all the CMS mandated APIs.
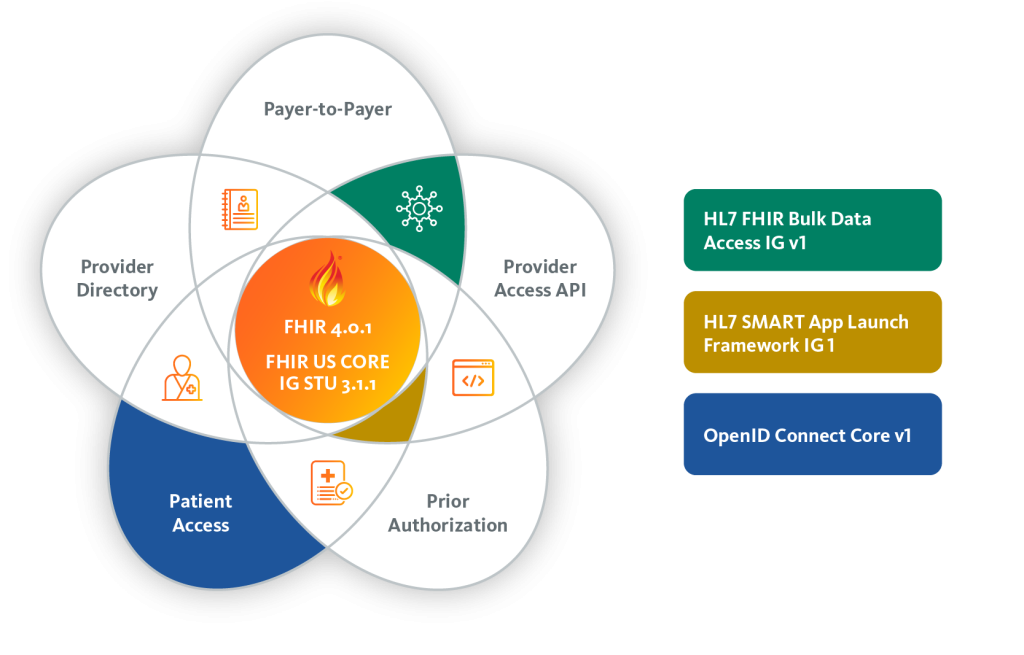
To create USCDI version 1 data, health plans will need a robust infrastructure,. This should nclude data standardization tools, interoperable electronic health record (EHR) systems, and capabilities for secure health information exchange. However, it’s important to know that some standards suggested by the Final Rule are still being finalized. Even if you have teams skilled in FHIR, building internally means keeping up with these evolving requirements.
Affected payers must furnish members with details about the Payer-to-Payer API. It is important to note that members are not obligated to make a decision within this one-week timeframe.
Should a member choose to opt in, impacted payers are mandated to integrate any received data into the patient’s record. This integration plays a crucial role in promoting seamless care continuity as patients transition between different payers.
The process of sharing member data with a health plan involves a technical three-step sequence that involves authentication, member matching, and data retrieval. Without data exchange framework in place, payers may encounter challenges to information requests or handling data from other payers. This could raise privacy concerns and potentially result in delays in making critical decisions that rely on this data.
There are different methods to establish connections for payer-to-payer data exchange, each requiring various levels of effort. It is essential to evaluate your current capabilities and assess the available resources for supporting connectivity.
Building Internally: Organizations exploring internal development should consider the resources, cost, and time it takes to construct a connectivity system. During a meeting with our first Payer-to-Payer Data Exchange cohort, we interviewed a health plan representative. She shared that establishing a single connection with another payer required six to eight individuals and approximately six months to establish one connection. Similar efforts are expected for each following connection.
Pursuing connections without an experienced partner may be challenging, given the Final Rule’s requirements, the need for extensive collaboration, and potential increased effort for multiple connections. This is especially true when considering the associated expenses and the need for continuous tweaking as the market matures. Moreover, the ongoing maintenance of connections and the necessity to stay current with evolving standards, may diminish the perceived value of the internal resource investment.
Outsourcing: Instead of each payer building their own individual connections, health plans might consider collaborating with a centralized solution. While acknowledging the costs, many health plans find that outsourcing provides a swift and efficient solution, expediting the implementation process. Outsourcing may offer additional benefits. These benefits include leveraging vendor expertise, meeting compliance deadlines effectively, and ensuring a smoother transition into a state that can handle complex data exchange requirements.
How Availity Can Help: Availity has embarked on a dynamic partnership with a select cohort of payers to pioneer the establishment of a set of payer connections within our cutting-edge Connectivity Hub. The Connectivity Hub accelerates interoperability and streamlines the Payer-to-Payer API Data Exchange process. Our aim is to minimize the reliance on costly and time-consuming point-to-point connections. Download our eBook to learn more!
Ensuring effective communication with members is vital for promoting adoption. This is particularly true given the relative unfamiliarity of the CMS Interoperability and Prior Authorization Final Rule beyond healthcare circles. To encourage members to initiate the request, affected health plans must provide members with materials that outline the advantages of Payer-to-Payer API Data Exchange.
For instance, your health plan could create a one-page information sheet highlighting the advantages of opting into payer-to-payer data exchange. Users could then send this informational material alongside their initial enrollment paperwork. A link can be included that directs members to a site where they can provide consent. By incorporating this information into their enrollment process, you ensure compliance with the requirement to provide details within a week of enrollment commencement.
Subsequently, sending out additional communications post-enrollment serves to reinforce the educational resources that were previously provided and eliminates the risk of missing the one-week timeframe for information dissemination. These materials should include clear instructions on how members can opt in or withdraw their previous opt-in decision. Additionally, effective customer service representatives. Armed with scripts and a well-defined process, can also play a pivotal role in assisting both current and past members in accessing their data through the Payer-to-Payer API.
In conclusion, while the establishment of connections with payers demands technology, personnel, and resources, the substantial benefits derived from seamlessly transferring medical records with members as they transition to a new health plan outweigh the associated efforts. The enhanced continuity of care and improved access to comprehensive health data contribute significantly to the overall well-being of individuals within the healthcare ecosystem.
If you’re interested in learning more about our Payer-to-Payer Data Exchange cohort, check out our latest white paper. This resource will give you a deeper dive into hidden pitfalls and progress achieved throughout implementation and end-to-end testing.
Michael Taylor, Senior Clinical Product Owner at Availity, has over a decade of experience in Health IT. He has successfully navigated roles such as Interoperability Engineer, HL7 Analyst, Product Manager, and Senior Product Marketing Manager. His expertise spans a wide range, including FHIR provider directories, social determinants of health, and electronic consent management.
Outside of his professional life, Michael enjoys hiking and kayaking. One of his favorite pastimes is modifying and playing with foam blasters (kid’s Nerf toys), dedicating time to enhance their performance and appearance, which showcases his unique blend of technical skills and creativity.

Michael Taylor
Senior Clinical Product Owner at Availity
1This article is for informational purposes only and is in no way intended to be legal or compliance advice. Consult with your legal and compliance teams for guidance on how the Interoperability and Prior Authorization Final Rule applies to your organization.
2Availity officially initiated its first cohort on August 22, 2023, and maintains regular meetings with participants to collaboratively address pivotal decision points.
3Please note, there are certain pre-qualifications required for a health plan to be considered for participation in a cohort.